
THERE IS SOMETHING oddly comforting about reading my father’s autopsy.
Maybe it’s the good news: “The skin is normal. The esophagus is without lesions. The stomach is unremarkable. The small intestines contain mostly undigested food particles.” Even quitting smoking 17 years before had paid dividends: “There’s only mild emphysema.”
Or perhaps it’s the good that came out of it: “The patient had most organs donated, including kidneys, heart valves, liver, eyes, parts of spleen and lymphatic tissue, bladder, prostate, and most of pancreas.”
My father’s death, we know from the Center for Organ Recovery, ultimately improved the lives of a half-dozen men and women in the Northeast.
Or maybe, probably, it’s that it brings me back to the exact moment in time when everything changed. His life, suspended instantly. Mine, altered forever. Yet I feel a sense of potential. Of what might have been had he been holding the railing, as Mom instructed twice. Of how things might have gone differently had we understood what was happening inside his brain that day, or even over the previous five years. Or, frankly, if anyone in the family had bothered to wonder what killed his aunt and two uncles, brought his grandmother to stare-into-space dementia, and put his own mother in a nursing home six years before, where she lay that fateful day unable to speak or move.
Advertisement – Continue Reading Below
I pore through the document over and over, 59 years of humanity summed up and single-spaced on a wholly insufficient five pages, and feel like I’m getting closer. To him. To it—the mystery of what killed him. Because the clinical explanation—”massive intracerebral hemorrhage”—doesn’t begin to tell the story. It just deepens a mystery that’s three generations old and counting.
My dad fell, backward, down eight stairs. He hit his head on a slate landing. Hard. This opened as many as three dozen bleeding wounds in his brain: hemorrhagic strokes. But it’s not that simple. Can’t be. Was there a tie-in to those excruciating back pains he’d been having for three decades? What about the fact that his right leg would just collapse sometimes? He’d be standing in the middle of the yard, and just fall. Was the ministroke he’d had 2 years before a contributing factor? And could it be a coincidence that his uncle George, a decade before him, suffered a parallel set of stroke symptoms and an even more tragic death?
And then, what about this note, buried in the autopsy’s addendum: “Findings are consistent with, but by themselves not diagnostic of, Cadasil.”
What the hell is Cadasil?

CHANGES ARE, YOU know someone who’s had a stroke. As diseases go, stroke is the third-leading killer of men in the United States, behind heart disease and cancer. This year, 700,000 Americans will have one, and a fourth of those will die. Another third will be permanently disabled. And don’t think it can’t happen to you: One in 12 victims is under age 50, and almost one-third succumb before their work lives are finished.
There are two types. Ischemic strokes, which are caused by a blocked blood vessel, make up around 80 percent of all strokes. Hemorrhagic strokes make up the other 20 percent; they occur when a vessel tears and blood leaks into the brain.
My dad’s mini-stroke—diagnosed in March 1997, at age 57, two years before his fall—was ischemic. He went to his doctor complaining of lack of balance and of weakness on his right side. An MRI scan revealed a “small infarct”—the stroke—in his left cerebellum, the part of the brain responsible for coordination. But in his medical records, the doctor also noted “moderate lacunar infarcts”—that’s doc-speak for a series of so-called silent strokes.
Advertisement – Continue Reading Below
“Most people think of a stroke as a catastrophic event,” says David Liebeskind, M.D., an assistant professor of neurology at the UCLA stroke center, the country’s foremost stroke treatment and research facility, “but more than 11 million people will suffer a silent stroke this year.” That’s roughly one in every 25 Americans, mostly men. “A single silent stroke may not cause any symptoms,” adds Dr. Liebeskind, “but over time, silent strokes chip away at your ability to function.”
It happens when a tiny clot—maybe a piece of plaque that breaks from a vessel in your arm or leg—meanders its way to the brain and plugs up a capillary, preventing oxygen-rich blood from reaching the tissue on the other side. Almost instantly, a dime-size part of your brain dies.
You, however, feel fine. You don’t even know it happened, so you don’t change your lifestyle to reduce your risk of another. A couple of years later, it happens again. Then again a few years after that. Soon you can’t spin a basketball on your finger anymore. Maybe you become frustrated because you keep forgetting the punch line to a joke you’ve been telling for years. Your balance isn’t what it used to be, either, and you can’t always find the right word. Suddenly, you’re 65 and your grandkids think you’re losing your marbles. You actually have been for years, one by one.
 COURTESY OF WILLIAM G. PHILLIPS
COURTESY OF WILLIAM G. PHILLIPS
Advertisement – Continue Reading Below
“It’s called vascular dementia,” says Dr. Liebeskind. “It’s the second most common cause of dementia, behind Alzheimer’s disease. You don’t know it’s happening until you’re older. But if you pulled a hundred 40-year-olds off the street and did MRI scans of their brains, you’d see that a large number have already had a silent stroke.”
Maybe that explains why my dad almost drove us off Mount Washington once. It was in 1995, two years before he suffered his mini-stroke. We were above the treeline, heading down; he was driving, I was in the front passenger seat, and a vanful of family rode in the back. I noticed that he couldn’t keep the vehicle in his lane. Twice, the front wheel edged off the rocky pavement to within feet of the cliff beside me.
“You okay, Dad?” I remember asking.
“Fine,” he snapped back. Then, after a pause: “Sure is windy, isn’t it?”
It was, and that was that. But my concern crystallized on the 360-mile trip back to New York—I felt like I was riding with someone who’d had one too many. I filed it under “Dad’s getting older.” I certainly didn’t think he might have suffered some sort of stroke. Had he suffered multiple silent strokes before the trip? Doctors can’t say—it’s impossible to date previous strokes that precisely. But now that I know the stroke symptoms, I have no doubt.
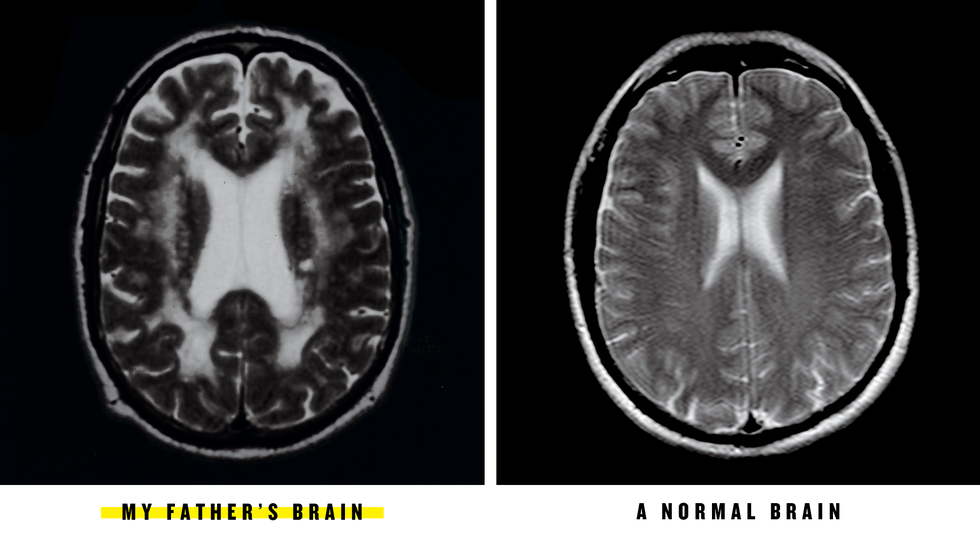
At the time of his MRI scan, the ministroke diagnosis was actually the good news—it was small and contained, and Dad was already regaining some of the lost function. But his doctor also noticed that the deep center portions of my father’s brain showed up as a bright white on the scan. He hadn’t seen anything like this before, at least not in a man so young.
These odd images were coming from the tissue—called white matter—that protects nerve fibers. Even more disturbing, large chunks of it were missing. This is not unheard of—white matter starts developing when you’re an infant and slowly begins to disappear in old age. But my dad wasn’t old.
Confounded, the doctor referred my father to a neurologist at the University of Pittsburgh medical center. Two weeks later, my parents made the 80-mile journey.
My mother drove.
Advertisement – Continue Reading Below
“WE SHOULD SCAN your brain.”
That was my doctor talking to me two months after my father passed away.
“But . . . why?”
“We’ll get a baseline,” he said. “Then, when you’re older, we’ll be able to notice any changes in your brain.”
“But my father’s death was an accident.”
“You should have it done,” he insisted. “If not right now, then sometime soon.”
So I found a new doctor.
I was 29 when my father died. It was the best time of my life, I thought, what with my cool New York apartment, great New York job, and hip New York girlfriend who was taking time off so she could plan our wedding. Sure, my father’s death halted my stride a bit, made me think about mortality. But not my own. Despite all the evidence that my dad’s fall was caused by something more insidious than a simple loss of balance, for years I referred to his death as a “tragic accident.”
Fact is, I probably should have seen it coming the day before the fall.
On October 23, 1999, my fiancée’s parents flew in from Milwaukee to meet my family for the first time. They landed at LaGuardia, and we drove them to my sister’s place outside of Philly. The women congregated in the kitchen, discussing the rehearsal dinner and the receiving line, and ways to turn the hall completely periwinkle. The men hunkered down in the family room, watching the Penn State football team heroically come back and defeat Purdue, 31–25.
We talked fishing, too. Nothing odd here. It was Dad’s passion since he’d retired six years before. Of course, I use the word “passion” in a relative sense; fishing was one of just two ways my dad passed the time in retirement. The other: sitting in front of the TV, most of the time (thankfully) with it on.
Advertisement – Continue Reading Below
 COURTESY OF WILLIAM G. PHILLIPS
COURTESY OF WILLIAM G. PHILLIPS
caption tk
Looking back, this appalls me. My dad once told me, after visiting his own aging father, “If you ever find me sitting in front of the TV day after day like that, promise you’ll just shoot me.” But it was easy to forgive in my father. Before retiring at age 52, he had spent 17 years, 14 hours a day, 7 days a week, running a small general store in a wilting Pennsylvania town, turning it into a hugely profitable operation. The man deserved a break. He got it with a TV remote, or a rod and reel, in his hand.
He told his fish story that day, and we indulged him.
“So I pulled it in,” he said with jerky rod-and-reel hand motions, “and it was another of those damn . . . ah . . . those . . . ” He excused himself, went into the kitchen, and quietly asked my mom for the name of the fish he always caught. He nodded and headed back to the family room, but stopped halfway, turned around, and went to Mom a second time. “It’s called a crappy,” she told him again.
That evening, we all went into town to watch my nephew ride with his Boy Scout troop in a Halloween parade. We parked a few blocks from the parade route. As we walked toward it, my dad was limping, grimacing. During the parade, he leaned against a telephone pole 10 feet behind us. He never saw his grandson ride by. He didn’t seem to care.
Advertisement – Continue Reading Below
After the parade, we said our goodbyes with no idea just how final they’d be. My parents left my sister’s the following afternoon. On the four-hour trip home—my mom driving, of course—my dad barely said three words. When they reached home, they entered through the basement. My dad grabbed an overnight bag and started upstairs. My mom was right behind him. On the third step, he fell backward. My mom caught him. “Bill, hold on to the railing,” she warned. He didn’t respond. On the seventh step, he fell back again. Again, my mom caught and scolded him.
He dropped the luggage in the bedroom and went outside for the mail. My mom started unpacking. A few minutes later, she heard a thud. She ran to the steps. Mail was strewn about. My dad was lying on the landing on his back, legs completely straight, toes up, arms at his sides. This is called posturing; it’s a sign of a serious brain injury. He was unconscious but breathing. A rivulet of blood trickled out from behind his head. Mom called 911.
An hour later, around 7 p.m., back in New York, my phone rang. It was my sister. “Dad’s had a serious fall,” she began. “They’re flying him to a hospital in Pittsburgh.”
My fiancée and I packed quickly and headed for the car. I couldn’t bring myself to heed my sister’s last piece of advice, so I left my black suit hanging in the closet.
ON A COOL DAY this past May, I trace that route to Pittsburgh once again. My sense of urgency is different, but somehow the same. This time, I’m meeting with Clayton Wiley, M.D., the pathologist at the University of Pittsburgh medical center who interpreted my father’s autopsy. I get the sense he’d prefer not to be having this conversation, but that he acutely understands a son has a right to know.
“Are you squeamish?” he asks me.
“No, not really.”
Advertisement – Continue Reading Below
He reaches for his flat-panel computer screen and swings it my way, then double-clicks. A handful of images pop up, each showing a glob of pink tissue and coagulated blood. It looks like nothing in particular—a used placenta, maybe, or a GI’s abdomen after a grenade attack—but I know what’s coming.
“This is your father’s brain.”
He pauses to allow it to register, then proceeds: “As you can see, much of the brain tissue has been destroyed. These hemorrhages are not something a person could recover from. The blood clot in the center of the brain alone is 5 inches in diameter.
“Notice how soft the brain tissue is,” Dr. Wiley continues. “It’s softer than Jell-O. It can’t keep its shape. That’s an indication that the tissue lacks normal proteins. That it’s dead.” Of course it is. It’s sitting on a table. But I understand his point, that my father was brain-dead long before we pulled him off life support a day and a half after his fall.
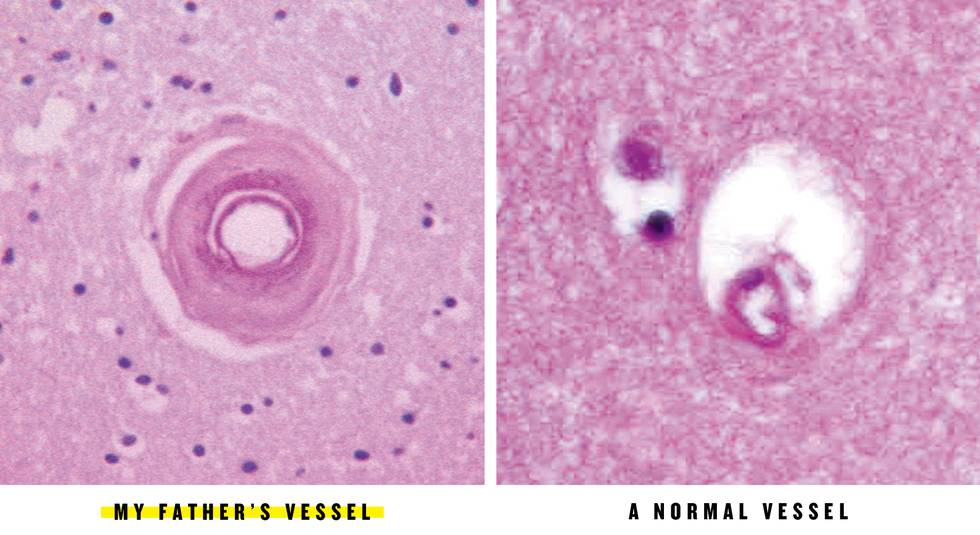
Dr. Wiley clicks open another file. “This is a microscopic image of one of the blood vessels in your dad’s brain.” If not for the purple tinge—dye makes it easier to pick up abnormalities—you could mistake it for a satellite photo of a hurricane. The “eye,” just a few microns in diameter, is the blood-vessel cavity. The wall around it is made up of dozens of swirls, as if the vessel were being tied up by kite string. The wall is roughly the same thickness as the hole where the blood is supposed to flow.
“We looked at these vessels because we wanted to see if there was anything in the brain that could explain the severe hemorrhages,” says Dr. Wiley. Blood-vessel walls should be thin. These are extremely thick. And when they’re thick, they start to constrict and harden. They’ll break like eggshells. This is what happens with hypertension. The vessels are pulsed by high blood pressure, and they thicken to accommodate the increased pressure. That’s how high blood pressure causes strokes.
Advertisement – Continue Reading Below
“But your father didn’t have high blood pressure, or any of the major risk factors, so something else caused the thickening.”
“Something like Cadasil?” I ask.
Dr. Wiley pauses again. “After he died, we did genetic testing for Cadasil,” he says. “The results were negative. But the tests are only 70 percent sensitive, and we’re discovering new variants all the time. I’d strongly suspect Cadasil. Maybe even a variant that hasn’t been seen before.”
Cadasil is a disease first discovered in a French family in the 1950s. In the mid-’90s—around the time of my father’s ministroke, in fact—it was linked to mutations in a gene called Notch 3, which lives on chromosome 19. Though the mechanism is unclear, the bad gene causes granules of protein to be deposited in the walls around the brain’s blood vessels (and, to a lesser extent, throughout the body). This thickening constricts the vessels and makes them brittle, leading to migraines, mood changes, depression, strokes, and, eventually, Alzheimer’s-like dementia.
Cadasil is still considered rare—it’s only been diagnosed in about 500 families worldwide—but since the first genetic test became available in 2000, it’s been showing up in every corner of the world. “In the end,” says Brad Worrall, M.D., M.Sc., an assistant professor of neurology at the University of Virginia who’s been studying the link between heredity and strokes for 10 years, “it’ll probably turn out to be the most common genetic cause of strokes.”
The disease tends to appear in middle age: On average, the first symptoms materialize around the age of 45, with the slow mental decline beginning shortly afterward. Most Cadasil patients don’t live to 70, though life expectancy varies widely. Even in the same family, says Dr. Worrall, it kills some members in their 20s and others in their 90s.
Dr. Wiley explains that because Cadasil is a so-called autosomal dominant disorder, only one parent needs to have the bad gene for it to be passed on to his or her children. “That means,” he explains calmly, “if your father had Cadasil, you have a 50 percent chance of having it, too.”
Dr. Wiley senses my discomfort. “But remember, what’s true in 2005 may not be true in 2010,” he says. “New therapies will come out. If I were you, I’d get a baseline brain scan done. With Cadasil, very specific white-matter patterns show up in MRIs decades before symptoms start, so you’ll know right away if you’re at risk. And even if it is Cadasil, there may be things you can do to prevent or delay it.”
Advertisement – Continue Reading Below
It’s the same argument my ex-doctor had made six years before, but—maybe because I’m older, wiser—this time it clicks. I e-mail Dr. Liebeskind for a second opinion. He writes back: “The UCLA stroke center is a world-leading institution in brain imaging. I can arrange for an MRI tailored to stroke and cerebrovascular disorders, if you wish.”
I book a flight to Los Angeles.
YOU ACTUALLY DON’T have a stroke. You develop one. Meaning: For each minute that passes, a tiny bit more brain tissue dies. This slow progression continues until all the downstream tissue starves to death or the blockage is cleared.
The tissue doesn’t die immediately because every major artery in the brain has a few smaller backups, vessels that pick up the slack when another becomes clogged. They’re called collateral vessels, and they’re the focus of Dr. Liebeskind’s research.
The problem with collaterals, says Dr. Liebeskind, is that they’re local roads. When a major interstate in the brain becomes blocked, the blood has to turn around, find the appropriate alternative pathway, then take the scenic route to the target destination: brain tissue that’s starved for nourishment. This circuitous route, however, largely strips the blood of its oxygen. Even so, the barely oxygenated blood can keep tissue functioning for a few hours; hence, the oft-repeated 3-hour window for reaching a hospital. (Capillaries don’t have an effective collateral network, which is why silent strokes kill brain tissue almost instantly.)
Dr. Liebeskind’s goal is to find ways to put more oxygen into the bloodstream, then divert more blood into collateral vessels. At Massachusetts General Hospital, doctors have been experimenting with giving supplemental oxygen to stroke victims. “It’s quite promising,” says Dr. Liebeskind, “but not the complete answer. The route matters, too.” So he—along with some of the world’s top stroke researchers—is working on therapies that could someday improve an at-risk patient’s collateral flow: drugs to make existing vessels larger, for example, or surgery to add new vessels to the brain.
Advertisement – Continue Reading Below
“We’ve already made huge strides in the past few years,” he says. “We’re able to bring people back from the brink of death. A person can’t speak or walk. We go in, open the vessel, and within seconds they can speak and walk again.”
THE FIRST MAJOR advance, a clot-busting drug called tissue plasminogen activator (tPA), was cleared by the FDA in 1996. It’s effective at dissolving most clots, but it also has a tendency to cause bleeding in the brain. For that reason, it remains controversial, though a 2004 study found that ischemic-stroke patients who received tPA were twice as likely to recover fully. Still, the 3-hour window is the stumbling block. “Patients are going to the hospital too late,” says Dr. Liebeskind, “so only two or three percent of stroke victims receive tPA.”
Last fall, another weapon was added to the neurologist’s arsenal when the FDA approved the Merci device, a wire corkscrew developed at UCLA that can be snaked into the brain to remove a clot. There’s a lot of excitement around Merci, says Dr. Liebeskind, because it’s been approved for use up to six hours after the onset of stroke symptoms. “Even in patients where it may have been too late in the past, reopening vessels can improve their long-term outcomes.”
Neither of these treatments, however, could have helped my father. “With small-vessel disease, like what your dad had, the only treatment is prevention,” says Dr. Liebes-kind. “Most strokes, around 60 percent of them, are brought on by high blood pressure, diabetes, high cholesterol, or obesity. The key is controlling your risk factors.”
 COURTESY OF WILLIAM G. PHILLIPS
COURTESY OF WILLIAM G. PHILLIPS
caption tk
Advertisement – Continue Reading Below
And if you have no risk factors? Like my father, like me? “That’s where the other 40 percent come in,” Dr. Liebeskind says. “You have to look at genetic factors, which may alter arterial walls or affect the tendency of your blood to clot. We’re slowly starting to understand the role of genetics. And once we identify the stroke-causing genes, we can develop specific treatments.
“Decades ago,” he continues, “no one thought there was anything you could do about stroke. Today, we’re on the verge of major breakthroughs.”
Already, says Dr. Worrall, researchers have identified two types of stroke-causing genes. “Probabilistic” genes may increase your risk of stroke, especially if you’re exposed to the wrong environmental factors. “Deterministic” genes, it’s believed, always cause the disease, though the age of onset varies greatly. Researchers are focusing on probabilistic genes now, because they’re more common and some—in conjunction with the right lifestyle choices—also seem to have the power to protect against the disease they cause.
One such gene has been linked to hardening of the arteries. “Preliminary research suggests that if you carry a mutated version of the gene and eat a diet rich in omega-6 fatty acids, your risk is much higher than the general population’s,” says Dr. Worrall. “But if you eat a diet rich in omega-3 fatty acids, your risk is lower than that of the general population.”
Notch 3, the gene linked to Cadasil, is thought to be deterministic, but it has so many mutations that no one knows for sure. Either way, it won’t affect the search for a treatment or cure. “The key with Cadasil is figuring out how the bad gene causes the protein deposits,” says Dr. Worrall. “If we can do that, we can figure out how to interrupt the process.” Several clinical trials in Europe, and one in the United States, are testing drugs that may do just that.
This knowledge certainly makes the idea of having a brain scan easier to accept, though Dr. Worrall offers a note of caution: “Because your family history is so striking, it’s reasonable for you to want to know what your risks are. But we can’t treat Cadasil yet. Do you really want to be tested for an incurable, relentlessly progressive disease you have no symptoms of?
“If the test comes back positive, have you thought about how you’ll react?”
Advertisement – Continue Reading Below
MY BRAIN SCAN is tomorrow, and I suspect the images will reveal traces of Dr. Worrall lodged in my gray matter.
I can’t get him out of my mind—in particular, one theory of medical diagnosis he mentioned.
He described it like this: “In medicine, we always try to explain a set of symptoms with a single cause. If your dad had come to me, I would have looked at the whole picture: the strokes, the white-matter changes, the leg and back pain—his high arches and clawed toes, too, which can indicate an underlying neurological disorder. Then I’d have tried to put it all together with a single diagnosis.”
That’s exactly what’s been bugging me: Nowhere in the medical literature has Cadasil been linked to leg and back pain, though several other disorders do manifest themselves with all of these symptoms. One is Carasil, a recently discovered cousin to Cadasil that’s inherited only when both parents possess the defective gene. Another is Mast syndrome, a rare type of hereditary paraplegia that my father’s uncle Bill was diagnosed with but was never actually tested for.
The more I ponder this, the more it feels like I may not know the enemy yet. Suddenly, I can see why Dr. Worrall told me the results of the MRI could be lose-lose.
“What if they spot something and you assume it’s Cadasil,” he said, “but you end up doing genetic testing and it’s not. It’s just . . . something. Where do you go from there?
Advertisement – Continue Reading Below
“And what if they see nothing? You think you’re free and clear. Maybe you won’t watch your blood pressure as closely, or your cholesterol. You’re just setting yourself up for a stroke later on.”
“What would you do?” I asked him.
“Find out definitively what happened to your dad first,” he said. “You mentioned they saved his brain tissue—you can test it for anything. If a relative develops symptoms, maybe he or she can be tested. Once you know what’s in the family, then you can decide whether you want to be tested.”
A reasonable approach, surely. But in the end, it’s my 2-year-old daughter, Lindsay, who unwittingly seals the decision. She’s napping as I pack for Los Angeles. Before I leave for the airport, I wake her up, tell her that Daddy is going away for a couple of days, and hold her close for a few minutes.
I can’t help but wonder: Will she have to make a call someday like my sister did, to tell her sister—that Dad’s had a serious fall? Will she herself, like my great-aunt Olive, have to write a goodbye letter to family someday in anticipation of a slow, progressive demise?
She looks up at me as I wipe away a tear. “Daddy, will you play with me when you get back?”
“Of course I will, honey.”
At that moment, I decide to cancel the MRI. I don’t want to come home a different man, a dying man. I will identify the enemy first. Two days later, I have my father’s brain-tissue samples sent to UCLA for testing, and, as I write this, the nation’s top stroke researchers are on the case. It may take months. It may take years. I will watch and wait.
And live.
Update: April 9,2024
I’M PLEASED TO report the murderer has been found. Ten years ago, my dad’s younger brother became the first family member officially diagnosed with Cadasil. Uncle Bob turns 80 this year and while the disease has ruthlessly stolen his mobility, it hasn’t taken his sly grin or devious demeanor.
Cadasil is still considered a rare disease, but it’s far more common than previously thought. When I began my manhunt in 2005, there were only 500 cases in the world. Today, there are as many as 400,000. It even made a cameo last year as the main character’s affliction in Netflix’s Fall of the House of Usher. There’s still no cure. The disease is progressive, debilitating, and unstoppable.
You might be wondering: Have I been tested? No, I haven’t. After writing “Hunting My Father’s Killer,” I wrestled with this decision for years. For me, it comes down to this: I have no symptoms (*knocks on wood*). Should I ever develop them, I’ll absolutely get tested. But until then, I’d rather live with a killer in my midst than know for certain I’m his next victim.
The disease may be a curse but the story has been a gift: It’s brought me closer to my father, who hid so much pain from me. It’s compelled me reconnect with extended family and collectively dive deep into our genealogy. But above all, it become an ever-present reminder to embrace all of life’s possibilities — every day — with intention, urgency, and action.
{kind=link}